What are the other Names for this Condition? (Also known as/Synonyms)
- Bile Duct Stone
- Common Bile Duct Stone
- Gallstone in the Bile Duct
What is Choledocholithiasis? (Definition/Background Information)
- Choledocholithiasis is the presence of stones (gallstones) in the common bile duct (CBD). The presence of even one stone in the CBD is called Choledocholithiasis
- The liver is located on the upper right side of the abdomen. Among other functions the liver produces bile, which is important for the digestion of fat
- The bile comes out of the liver through the common hepatic duct (hollow tube) and enters the gallbladder through the cystic duct
- The gallbladder is a small sac located under the liver and its main function is to store bile and release it, as and when it is required
- The cystic duct joins the common hepatic duct to form the common bile duct
- The common bile duct carries bile into the duodenum (gastrointestinal tract). Bile in the gastrointestinal tract helps in the digestion of fat
- The gallstones are made up of a mixture of bilirubin, calcium, and cholesterol. There are 4 types of gallstones
- Cholesterol stones (the most common type)
- Pigment stones – black: These stones are commonly found in individuals with hemolytic (destruction of red blood cells) anemia
- Pigment stones – brown: These stones are commonly seen in Asians and are thought to arise due to infection of the bile duct. These type of stones are commonly formed in the common bile duct than in the gallbladder
- Mixed stones: Contains a mixture of the above stone types
- The process of gallstone formation in the gallbladder is called cholelithiasis. Some of the stones exit the gallbladder and gets trapped in the CBD to cause Choledocholithiasis (secondary stones). Up to 15% of individuals with gallstones (cholelithiasis) have associated Choledocholithiasis. Uncommonly, stones may be formed within the common bile duct itself (primary stones)
- Choledocholithiasis may cause no symptoms or cause symptoms such as right upper abdominal pain, jaundice, etc.
- The treatment options for Choledocholithiasis include the removal of the stones and removal of the gall bladder. The prognosis (outlook) is generally good with prompt diagnosis and early treatment
Who gets Choledocholithiasis? (Age and Sex Distribution)
- Any individual who has gallstone disease (cholelithiasis) is at risk for Choledocholithiasis (or Gallstone in the Bile Duct). It is more common in the elderly adults, than in children or younger adults
- Gallstone formation is more common in women than men
- Cholesterol gallstone formation is more common in certain regions where there is high intake of dietary fat, such as in northern Europe, US, etc. Pigment gallstones-brown type formation is more common in Asia
- Cholesterol gallstone formation is common in Native Indians than other races or ethnicities
- Pigment gallstones-black type formation is more common in African-Americans than other races or ethnicities
What are the Risk Factors for Choledocholithiasis? (Predisposing Factors)
The risk factors of Choledocholithiasis include:
- Individuals who have had their gallbladder removed (cholecystectomy) are at risk to develop Choledocholithiasis
- Any individual with a history of gallstone disease (cholelithiasis) is also at risk to develop Choledocholithiasis
The following are the risk factors for gallstones formation:
- Cholesterol gallstones: These gallstones are formed whenever there is too much cholesterol in the bile. The risk factors are:
- Women gender (due to estrogen)
- Obesity
- Diabetes mellitus type 2
- History of Crohn’s disease
- Individuals with metabolic syndrome that includes insulin resistance, high blood sugar, obesity, low blood levels of good cholesterol (HDL), and high blood levels of triglycerides
- Rapid weight loss with extreme calorie and fat restriction
- Rapid weight loss followed by quick weight gain
- Gastric bypass surgery performed for weight reduction purposes
- Organ transplantation
- High consumption of simple carbohydrates
- High levels of triglycerides in blood
- Decreased physical activity (and fitness)
- Pregnancy
- Conditions causing stasis of bile in the gallbladder
- Native Indians are at risk due to LITH genes, which increase fat storage
- Mutation in ABCG8 gene function increases one’s risk because excess cholesterol is pushed into the bile
- Use of medications, such as estrogens (oral contraceptive pill), hormone replacement therapy (used in postmenopausal women), clofibrate (used for treating high triglyceride levels), somatostatin, thiazide diuretics, etc.
- Prolonged intravenous feeding (used when an individual cannot take anything by mouth) increases one’s risk of getting gallstones
- Individuals with increased red blood cell destruction, such as hemolytic anemias, are at increased risk to get pigment gallstones-black type. Individuals with scarred liver (cirrhosis) are also at risk
- Individuals of Asian origin along with associated infection of the bile ducts, are at an increased risk to get pigment gallstones-brown type
- There are other unknown genetic and environmental factors, such as inflammation, infection, etc., which increases one’s risk of gallstones
It is important to note that having a risk factor does not mean that one will get the condition. A risk factor increases ones chances of getting a condition compared to an individual without the risk factors. Some risk factors are more important than others.
Also, not having a risk factor does not mean that an individual will not get the condition. It is always important to discuss the effect of risk factors with your healthcare provider.
What are the Causes of Choledocholithiasis? (Etiology)
Choledocholithiasis occurs due to one of the two mechanisms outlined below:
- Gallstones formed in the gallbladder move out and get trapped in the common bile duct (CBD)
- Stones that get formed within the common bile duct itself, which is seen in individuals without a gallbladder (which was surgically removed through a procedure termed cholecystectomy) and in individuals with bile duct infection
There are four types of gallstones. Each type is formed due to various reasons:
- Cholesterol gallstones are formed when there is too much cholesterol (super-saturation) in the bile. The factors that may increase cholesterol levels in the bile include estrogen (women), obesity, high levels of triglycerides in blood, genetic factors (such as in Native Indians), diabetes mellitus 2, etc.
- Pigment stones-black type (calcium bilirubinate): Bilirubin, a yellow pigment derived from breakdown of heme (present in red blood cells) tends to form insoluble jet-black pigment stones along with calcium
- Pigment stones-brown type: Bile is normally sterile, but in some unusual circumstances it may become colonized with bacteria. Bacteria break down lecithin (present in the bile) to release fatty acids which bind with calcium and precipitate to form brown pigment stones
- Mixed stones are mixture of cholesterol stones and black stones (calcium bilirubinate)
What are the Signs and Symptoms of Choledocholithiasis?
Choledocholithiasis (Gallstones in the Common Bile Duct) and cholelithiasis (with or without infection of the gallbladder) frequently coexist. The signs and symptoms of Choledocholithiasis and cholelithiasis include:
- Biliary colic: This is characterized by pain in the right upper abdomen (quadrant). The pain usually comes and goes, but sometimes it may be constant. The pain may be cramping or dull in nature. The pain may travel to the right shoulder tip or to the back. The pain may be worsened after having a heavy fatty meal
- Jaundice
- Clay-colored stools
- Nausea and vomiting
- Loss of appetite
- Fever with or without chills
- Tenderness of the right side of upper abdomen
- Liver enlargement
How is Choledocholithiasis Diagnosed?
The following procedures may be used to diagnose Choledocholithiasis:
- Thorough evaluation of the individual’s medical history and a thorough physical examination including the abdomen and skin
- During history-taking the physicians may want to know the following:
- When the symptoms began and whether they are becoming worse
- List of prescription and over-the-counter medications currently being taken
- About one’s personal and family history of gallbladder diseases, diet history, etc.
- Consultation with a gastroenterologist may be necessary, as they are the experts in dealing with such health conditions
- Stones in the common bile duct are detected using the following methods:
- Abdominal ultrasound: It is a noninvasive and inexpensive test that is also safe during pregnancy
- Endoscopic ultrasound or laparoscopic ultrasound may be used to better characterize the stones and the biliary duct
- CT scan of the abdomen is useful in diagnostic challenges to characterize complications of gallbladder or bile duct disease
- Endoscopic retrograde cholangiopancreatography (ERCP) permits radiographic imaging of bile ducts. It is the best test because it can help diagnose and the same time help remove a stone from the common bile duct. It is also helpful to visualize any associated pancreatic disease
- PTC (percutaneous transhepatic cholangiography) may be the modality of choice when performing ERCP is difficult
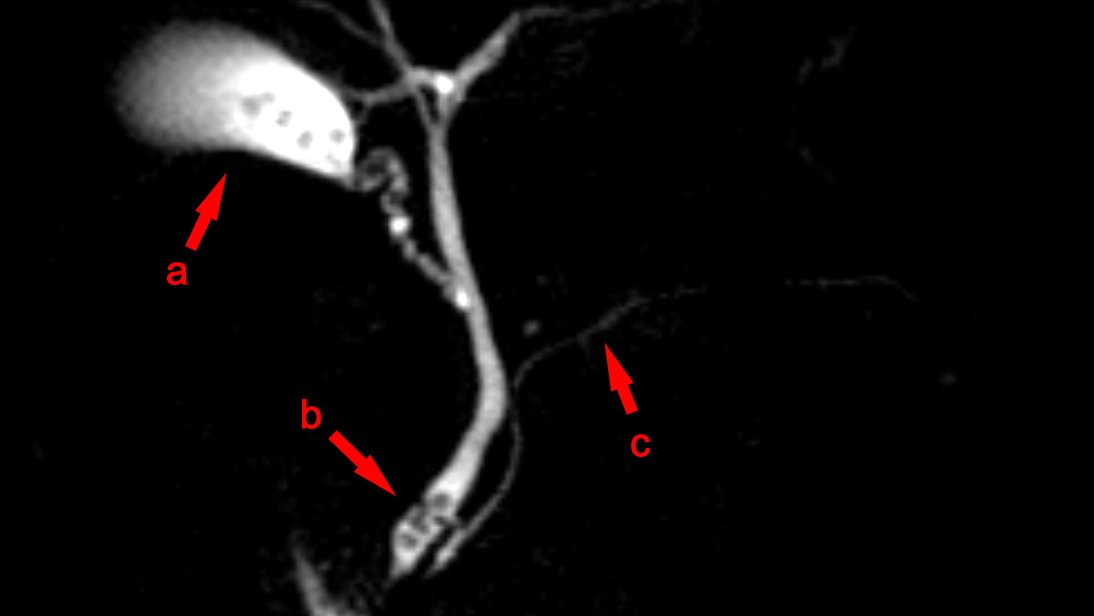
- MRI or MRCP (magnetic resonance cholangiopancreatography) is a good, non-invasive test to detect stones in the biliary tree
- HIDA scintigraphy is a good test to detect cystic duct obstruction (cystic duct and hepatic duct join to form the common bile duct), and analyze how the bile is flowing through the liver, gallbladder, and biliary tree
- Other tests that may be required in Choledocholithiasis to rule in or rule out associated diseases. They include:
- Complete blood count with differential, liver function panel (bilirubin, transaminases [ALT, AST], alkaline phosphatase, protein), blood cultures, amylase, lipase, prothrombin time, etc.
Many clinical conditions may have similar signs and symptoms. Your healthcare provider may perform additional tests to rule out other clinical conditions to arrive at a definitive diagnosis.
![choledocholithiasis-obstructive-jaundice-7-638[1]](http://lifewithnogallbladder.com/wp-content/uploads/2017/12/choledocholithiasis-obstructive-jaundice-7-6381.jpg)
What are the possible Complications of Choledocholithiasis?
The complications of Choledocholithiasis include:
- Cholangitis: Whenever the bile duct is obstructed the bacteria from the intestine may ascend up and cause infection of the bile ducts and beyond
- Secondarily biliary cirrhosis: Long-standing obstruction of the common bile duct can cause inflammation, destruction, and scarring of the smaller bile ducts inside the liver and cause liver failure
- Pancreatitis (inflammation of the pancreas) can occur whenever there is obstruction of the distal part of the common bile duct
- Gallstones ileus: Sometimes, the gallstone might reach the intestine and cause an obstruction
- Associated cholelithiasis (stones in the gallbladder) can cause acute cholecystitis (infection of the gallbladder)
How is Choledocholithiasis Treated?
Stones in the Common Bile Duct (Choledocholithiasis) should be removed, even if there are no symptoms. The stones may be removed by one of the following methods:
- Endoscopic sphincterotomy when an ERCP is performed
- Simultaneous bile duct exploration when a laparoscopic cholecystectomy (removal of gallbladder) is performed
- Balloon dilation of sphincter of Oddi, which is the site where the common bile duct attaches to the duodenum. This is usually reserved for individuals who have the tendency to bleed
- Endoscopic ultrasound-guided drainage along with percutaneous trans-hepatic cholangiography (PTC) is done in individuals, if endoscopic sphincterotomy is not able to remove the stones
- If the stone is large enough, then procedures such as lithotripsy (shockwaves to destroy stones), cholangioscopy (direct visualization of bile duct), or biliary tract stenting (placement of hollow tube) may be attempted at first
- If there is an associated bile duct infection, then antibiotics may be given.
How can Choledocholithiasis be Prevented?
The preventative measures of Choledocholithiasis include:
- Prevention of gallstone formation in the gallbladder through:
- Low-fat diet
- Exercise
- Overweight individuals, if planning to lose weight should decrease their weight gradually, but by meeting appropriate nutritional requirements
- Replacing saturated fats (animal fat) with monounsaturated fats (example olive oil) or omega-3 fatty acids products (example flaxseed, fish oil)
- Scientists believe that the consumption of coffee, fruits, vegetables, nuts, and high fiber may prevent gallstone formation
- Removal of gallstones formed in the gallbladder
- The gallbladder may be removed (cholecystectomy), if there is associated symptomatic gallbladder disease, or if the gallstones are more than 3 cm in size, or calcification (calcium on the gallbladder wall) is observed. A laparoscopic cholecystectomy is preferred over an open cholecystectomy
- Ursodeoxycholic acid medication can be used to dissolve the stones in selected individuals who refuse cholecystectomy
- Treatment of infections affecting the biliary tree (bile carrying ducts)
- Treatment of associated conditions that trigger gallstone formation
What is the Prognosis of Choledocholithiasis? (Outcomes/Resolutions)
- With prompt diagnosis and treatment Choledocholithiasis has a favorable diagnosis
- However, if diagnosis and treatment is delayed, it can cause complications and even lead to life-threatening situations
Additional and Relevant Useful Information for Choledocholithiasis:
Novel procedure Natural Orifice Transluminal Endoscopic Surgery (NOTES) for cholecystectomy is currently under review by the research community.
What are some Useful Resources for Additional Information?
American College of Gastroenterology (ACG)
4900 B South, 31st St. Arlington, VA 22206
Phone: (703) 820-7400
Fax: (703) 931-4520
Website: http://www.acg.gi.org
References and Information Sources used for the Article:
Nlm.nih.gov. Choledocholithiasis: MedlinePlus Medical Encyclopedia. 2015. Available at: http://www.nlm.nih.gov/medlineplus/ency/article/000274.htm. (accessed on 5/5/2015).
Papadakis M, McPhee S, Rabow M. Current Medical Diagnosis & Treatment 2015.; :699-705.
Helpful Peer-Reviewed Medical Articles:
Attasaranya S, Fogel E, Lehman G. Choledocholithiasis, Ascending Cholangitis, and Gallstone Pancreatitis. Medical Clinics of North America. 2008;92(4):925-960. doi:10.1016/j.mcna.2008.03.001.
London: National Institute for Health and Care Excellence (UK). Diagnosis and management of cholelithiasis, cholecystitis and choledocholithiasis. http://wwwncbinlmnihgov/pubmedhealth/. 2014. Available at: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0070643/pdf/TOC.pdf. Accessed February 5, 2015.
Chandran A, Sivarajan R, Srinivas M, Srinivasan V, Venkataraman J. Risk factors for choledocholithiasis in a south Indian population: A case–control study. Indian Journal of Gastroenterology. 2013;32(6):381-385. doi:10.1007/s12664-013-0354-x.
Reviewed and Approved by a member of the DoveMed Editorial Board
First uploaded: May 28, 2015
Last updated: Aug. 4, 2016
Source: https://www.dovemed.com/diseases-conditions/choledocholithiasis/
